Orthopaedic surgery involves the bones and joints and covers a very wide range of procedures.
I carry stock of 1.0mm, 1.2mm, 1.3mm, 1.5mm, 1.7mm, 2.0mm, 2.4mm, 2.7mm, 3.5mm, 4.5mm and 4.5mm broad conventional plates and screws and locking plate and screws in 1.5mm, 2.0mm, 2.4mm, 2.7mm and 3.5mm sizes alongside various external skeletal fixation options and dental acrylic for composite dental splints. This enables me to tackle the vast majority of fractures I'm likely to come across in cats and dogs of all sizes.
Fracture Surgery Gallery

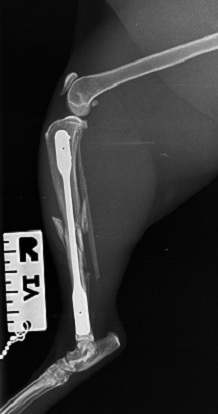
Feline tibia-fibula fracture, pre-op.

Feline tibia-fibular fracture, minimally invasive repair using a
LokRod plate of my design.

Feline tibia-fibular fracture, immediate post-op following LokRod repair.


Feline lateral maleollar (distal fibular) repair using a 0.7mm pin and wire

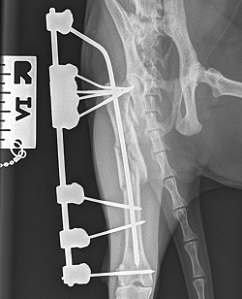
Feline femoral fracture repaired using a tied in external fixator with cluster pin technique in the proximal femur
Patellar Luxation Surgery
Patellar luxation is one of the two most common surgical conditions affecting the bones and joints in cats and dogs.
Patellar luxation is defined by the knee-cap (patella) sitting or popping out-of-place from the groove it would normally sit in. This most commonly occurs to the inside (medial) of the leg in small breed patients and to the outside (lateral) aspect of the leg in larger patients. With the altered biomechanics, it will also result in poor force-transfer through the limb, reducing the ability of the patient to lead as full and active a life. Painful cartilage wear occurs very commonly if left untreated, so early intervention is typically advised.
Surgery normally involves deepening the groove to better retain the patella, patella re-alignment within the groove by moving the attachment of its tendon to the tibia medially or laterally and tightening the tissues around the joint to help maintain the patella within its groove.
In extreme cases, in may be necessary to cut and straighten the femur, but thankfully this is pretty rare.
Cruciate Ligament Surgery
Cruciate ligament rupture is the other of the two most common surgical conditions affecting the bones and joints in cats and dogs.
Viewed from the side, the two cruciate ligaments (cranial/anterior and caudal/posterior) cross each other deep inside the joint. The cranial cruciate ligament runs from the back of the femur towards the front of the tibia and the caudal cruciate ligament runs from towards the front of the femur towards the back of the tibia. Most commonly it will be the cranial cruciate ligament that fails and this allows the femur to slip backwards down the natural slope on the top of the tibia. This results in lameness for a number of reasons such as instability reducing confidence in using the limb, pain from stretching any remaining cruciate ligament fibres, abnormal contact dynamics within the joint and potentially injury to the cartilage pads within the joint (menisci) which serve to increase the contact area between and cushion contact between the femur and tibia.
The first step of surgery is to remove remnants of the ruptured ligament and address any further damage within the joint, frequently this will involve removal of a portion of one of the menisci.
In dogs, there are now two main groups of options to stabilise the joint:
1) Ligament replacement. Several techniques are possible, but my preference is to use a modification of the lateral suture (lateral button suture or Isotoggle). I tend to limit their use to lighter patients, older or less active patients, patients with only a modest slope on the top of the femur and for patients where funds are limited. Each patient is an individual and decisions as to the most appropriate technique to use are still made on a case-by-case basis.
2) Geometric correction. This involves cutting the bone to change the geometry and reduce the influence of the slope on the top of the tibia in forcing the femur backwards as the patient stands. The patient's muscles then have to work less hard to keep the joint stable. I am by nature a conservative surgeon and it took me a long time to come to terms with cutting the bone to compensate for a ligament injury, however, there is no escaping that these techniques tend to work extremely well with post-operative comfort far better than you might expect. I advise geometric correction for the vast majority of patients.
In immature patients there are also options to either tighten the structures at the side of the joint as a temporary measure to improve stability until the patient is sufficiently mature to perform a more definitive repair or to place a screw across growing area the front of the tibial slope in the hope that it will grow more at the back than at the front, making it less steep - this procedure is sometimes known as a dynamic TPLO, but the results can be a little unpredictable.
In cats, cruciate ligament rupture it is almost always associated with trauma and will often involve other structures such as rupture of other ligaments around the joint. The surface at the top of the tibia that the femur sits on is more curved in cats than in dogs, such that it does not lend itself quite so well to geometric correction. Rupture of other ligaments around the joint complicates matters. The good news is that most cats respond very favourably to ligament replacement and this would be my preference in most cases.
Femoral Head and Neck Excision
Where there has been significant trauma or disease in this region and total hip replacement (THR) is inappropriate, femoral head and neck excision (FHNE) can be performed as a 'salvage' procedure. FHNE is the removal of the ball of the hip joint and a small area below this at the top of the femur. The intention is to reduce discomfort associated with the hip joint and it will often allow 'near normal' locomotion, especially in smaller patients.
Peak force and power generation with FHNE will be lower than for THR and the muscles tend to tire more quickly and so for larger and more active patients, THR will normally present the better outcomes, but at a price. I do not offer THR.
Open Reduction of Joint Dislocation
Several joints may become dislocated and surgery is often necessary to relocate the joint in a stable manner. Augmenting the joint by repairing or replacing the ligamentous structures around the joint may be required, especially in the hip, tarsus and elbow.
Arthrodesis
Arthrodesis is a salvage procedure that involves fusion a joint that is beyond repair or has collapsed because of muscle, tendon or ligament injury. Fusion is typically accomplished using plates and screws and I have been directly involved in the developing the range of arthrodesis plates available. Common joints to fuse include the tarsus and carpus, the shoulder and very occasionally the elbow and stifle. Depending on the joint affected, post-operative function is often very good and tends to be better for the lower motion joints.
Elbow Dysplasia
If the radius and ulna (the bones of the forearm) grow at different rates, the elbow joint will not form properly and the abnormal forces within the joint may result in damage to the joint, most commonly to an area on the ulna called the medial coronoid. Elbow dysplasia can be extremely uncomfortable. It can also be an extremely frustrating disease to manage as 100% correction of the abnormal forces within the joint is unlikely and arthritic changes are likely to occur with or without surgery.
Improving surgical procedures and implants to try and optomise the contact dynamics within the elbow is a big area of research within the veterinary orthopaedic community.
Angular Limb Deformity Correction
When angular limb deformities affect function or patient comfort, their correction is warranted. Although external skeletal fixation can be used to great effect, frame management can be a burden with frame related complications very common. These days, I tend to perform acute corrections where possible using plates and screws with no need for ongoing frame care.
What I don't offer
Total joint replacement, spinal surgery and arthroscopy (looking inside a joint with a camera) are arguably better performed in a dedicated referral environment, so are not services I currently offer.